Lab tests can be confusing when dealing with adrenal exhaustion. Some tests are useful. Others are not. In this article, I’d like to discuss these tests. I have no affiliation with any of the laboratories mentioned herein.
Let’s start with the fact that over 90% of SARDS dogs have elevated adrenal sex hormone steroids1. My own statistics put it close to 98%. This means virtually all SARDS dogs are dealing with elevated sex hormone steroids.
Here in the USA, there are two ways to evaluate adrenal sex steroids. These assays —each in their own way— give a fairly good picture of adrenal activity in SARDS dogs.
- The first is the Endocrine/Immune Panel at National Veterinary Diagnostic Services in Texas.
- The second is the Adrenal Sex Hormone Panel at the University of Tennessee.
Sometimes dog owners will try to economize and rather than using one of the panels mentioned above, will ask their veterinarian to run a serum estradiol and a serum (resting) cortisol test. These are straight blood draws that can be done locally. Practitioners outside the US, with few or no options to measure adrenal sex steroids, may also be tempted to run a serum estradiol or serum cortisol level.
In this article I’m going to explain why these latter two tests (serum estradiol, serum cortisol) are not very helpful in monitoring adrenal exhaustion. I’m also going to briefly discuss progesterone testing.
ESTROGEN — Why it’s pointless to measure serum estradiol alone
There are three main types of estrogen produced in man and dog. The first is called estrone or E1. Estrone production begins in the adrenal glands and concludes in fat cells, or brain, bone and skin tissue. Estrone (E1) is typically described as “adrenal estrogen”.
The second type of estrogen is called estradiol (E2). Estradiol is produced primarily by the ovaries. It can also be produced by the adrenal glands and the brain, but to a much lesser extent. Serum estradiol (E2) testing has been around for a while because of its role in reproductive health.
The third type of estrogen is called estriol (E3). It is primarily produced by the placenta during pregnancy.
Here’s the key point. The body readily converts estradiol (E2) to estrone (E1). And both can be converted to estriol (E3) ! So, at any given moment any of these estrogen levels can be in flux.
This is why a serum estradiol (E2) level is a poor indicator of adrenal exhaustion. First, because estradiol (E2) is primarily produced by the ovaries, rather than the adrenal glands. Second, the true estrogen load may “escape” a serum estradiol (E2) level, because at any given moment estradiol may be converted to another form of estrogen that is not being measured… not being tallied by the lab test.
A practitioner may assume all is well — because the serum estradiol (E2) level is within normal limits — when at the same time, estrone (E1, adrenal estrogen) may be elevated and simply unseen and unmeasured. It is the total estrogen load that’s important.
If an adrenal assay measures all three forms of estrogen it’s called a total estrogen level. This total value of estrogens provides a much more accurate picture than a sole estradiol level. This assay was once offered at National Veterinary Diagnostic Services (NVDS). And many of my previous papers refer to “total estrogen”.
In more recent years NVDS has fine-tuned their assay to evaluate only adrenal estrogen (estrone). An estrone level is also much more accurate than an estradiol level in evaluating this disease.
The second option with which to evaluate adrenal exhaustion is a lab panel that measures multiple adrenal sex hormones, as we see with University of Tennessee adrenal sex hormone panel. This provides a reasonable picture of adrenal activity.
Although the University of Tennessee panel only measures the estradiol (E2) component of estrogen, it measures additional sex steroids that occur in the adrenal pathway. If there is block in cortisol production, it’s typically evident somewhere in the pathway of sex steroids. So, while the University of Tennessee assay does not evaluate total estrogen, it makes up for it by measuring several additional sex steroids.
To recap:
- Estrone (E1) comes primarily from the adrenal glands
- Estradiol (E2) comes primarily from the ovaries
- Estriol (E3) comes primarily from the placenta
- The body can easily convert one form of estrogen to another, escaping a serum estradiol (E2) test
- A total estrogen level, or an estrone level, or a multi sex hormone panel provides a better picture than an estradiol (E2) level
Now let’s look at cortisol testing.
CORTISOL — A tricky trickster on paper
If you’ve read my work, you know that insufficient cortisol production results in an accumulation of adrenal sex hormone steroids. In humans, this has been documented for many decades. The cause? The body can no longer convert hormones called deoxycortisol into cortisol. Therefore, deoxycortisol levels accumulate. Think of it like water piling up behind a dam.
 Cortisol testing can be tricky to understand because the vast majority of lab tests, both veterinary and medical, are not very sensitive when it comes to measuring cortisol and its cousins. This means the tests cannot distinguish between cortisol and similar hormones like deoxycortisol. On paper, they’re all lumped together as “cortisol.” It’s called cross-reactivity.
Cortisol testing can be tricky to understand because the vast majority of lab tests, both veterinary and medical, are not very sensitive when it comes to measuring cortisol and its cousins. This means the tests cannot distinguish between cortisol and similar hormones like deoxycortisol. On paper, they’re all lumped together as “cortisol.” It’s called cross-reactivity.
In order to distinguish between cortisol and deoxycortisol, a lab must utilize either an electron microscope or a procedure called liquid chromatography. These techniques separate cortisol from deoxycortisol. Unfortunately, these procedures are unavailable in veterinary medicine and performed at few laboratories even in human healthcare.
To repeat, the average cortisol reading will lump together cortisol and deoxycortisol. They will both be labeled as “cortisol”. So, a dog could have very low cortisol levels, and very high deoxycortisol levels, and on paper the “cortisol” reading will be normal or even high.
Therefore, practitioners should understand that all cortisol readings — serum (resting) cortisol, cortisol post-ACTH injection, or cortisol post-dexamethasone injection — can demonstrate false readings due to cross-reactivity. Any one of these tests can lump together cortisol and deoxycortisol and thus produce a false normal or false high reading. This may lead a practitioner to believe these dogs are Cushingoid, when in actuality, the opposite is true. Elevated adrenal sex steroids typically result from low cortisol production.
Let me show you some examples. This paper describes the cases of five SARDS dogs tested with the University of Tennessee’s adrenal sex hormone panel. Initially, three of the dogs demonstrated high “cortisol” readings on paper. Some practitioners might assume these were Cushing’s cases. But as you’ll see, they were not.
All five dogs were treated with low dose cortisol replacement by their general practice veterinarians. The three high “cortisol” levels declined. In fact, there was a reduction in eight of the nine “cortisol” readings. To repeat: Low dose cortisol replacement caused the “cortisol” readings to decline.
Translation? These dogs weren’t really high in cortisol. The test was picking up deoxycortisol and including it in the “cortisol” reading. The low dose cortisol replacement reduced the brain’s stimulation of the adrenal glands. Consequently, deoxycortisol levels dropped and the “cortisol” reading dropped.
In a Cushing’s patient, low dose cortisol replacement would not have reduced the cortisol readings. SARDS dogs are not Cushing’s dogs. You can read more about that here.
Practitioners who are familiar with these cases do not focus on the cortisol reading until after about a year’s-worth of treatment. At that time, a year in, the cortisol reading it typically very low and reflects the true ability of the adrenal glands to produce cortisol, which is poor. Practitioners have the most success in managing these cases by monitoring total estrogen levels or other adrenal sex hormone levels.
To recap:
- Cortisol tests are not sensitive and lump together cortisol and deoxycortisol
- Dogs can have very low cortisol levels, and very high deoxycortisol levels, and on paper the “cortisol” reading will be normal or even high
- Cortisol levels are less important than total estrogen levels when assessing adrenal activity
PROGESTERONE — Why the reference range matters
In another article, I recently suggested that serum progesterone levels might be a viable option for those without access to the two adrenal panels we have here in the States. Progesterone is frequently elevated in cases of adrenal exhaustion. And progesterone demonstrates low cross reactivity with other adrenal steroids. In other words, serum progesterone levels don’t cause confusing results on paper (as cortisol can).
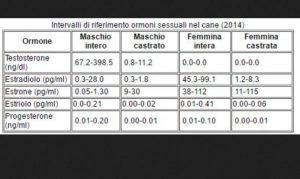
A veterinarian in Italy assayed the progesterone level in her SARDS patient, a neutered male. She used the reference range provided by the San Marco Veterinary Clinic and Laboratory, Veggiano, Italy. The SARDS dog’s progesterone level was significantly elevated at 0.39 ng/ml (normal = 0.01-0.10 ng/ml).
Please note that reference ranges at the San Marco Veterinary Laboratory (Table 1) have been determined for both male (maschio) and female (femmina) dogs, castrated (castrato) and intact (intera). This will fact will become important in just a moment.
Table 1. Sex hormone reference ranges, San Marco Veterinary Laboratory, Veggiano, Italy.

More recently, I’ve followed a SARDS case in South Africa where a serum progesterone level was also drawn. The dog was an intact female. According to the reference range provided from that lab, the dog’s progesterone was not elevated.
Why not? At the South African laboratory, progesterone levels are classified in terms of “active luteal tissue.” In other words, this reference range is designed to assess ovulatory status for breeding. It is not designed to evaluate small amounts of adrenal progesterone. That’s not a criticism, merely an observation.
Interestingly, when this dog’s result was evaluated against the reference range developed in San Marco, Italy (Table 1) the progesterone for this intact female translated to 0.21 ng/ml, or an elevated reading.
Progesterone can be measured by two scales. One is nanograms per milliliter (ng/ml) and the other is nanomols per liter (nmol/l). To convert nmol/l to ng/ml, we divide nmol/l by a factor of 3.18.
So, I now must add a caveat to my previous statement regarding progesterone. In order for a progesterone level to be useful, the reference range must be designed to measure adrenal progesterone rather than ovarian luteal progesterone. If it is not so designed, then the reference range in Table 1 may be useful to practitioners.
Someday, if veterinary medicine advances to the point of measuring 11B-hydroxylase type 1 or corticosterone as we do in human medicine, then laboratory testing may be less confusing. I hope this information has been helpful to you. These are complex issues. If you understood even a small portion of this article, you are now very knowledgeable about this topic.
In final review:
- The body can easily convert estradiol (E2) to estrone (E1), so a simple estradiol level is not useful in evaluating adrenal activity
- A total estrogen level or an estrone level or a multi sex hormone panel provides a better picture of adrenal activity
- Cortisol tests are not sensitive and lump together cortisol and deoxycortisol
- Dogs can have very low cortisol levels, and very high deoxycortisol levels, and on paper the “cortisol” reading will be normal or even high
- Cortisol levels are less important than total estrogen levels when assessing adrenal activity
- Serum progesterone levels may be more valuable IF the reference range is designed for adrenal production rather than ovarian activity
References
- Komáromy AM, Abrams KL, Heckenlively JR, Lundy SK, Maggs DJ, Leeth CM, MohanKumar PS, Petersen-Jones SM, Serreze DV, van der Woerdt A. Sudden acquired retinal degeneration syndrome (SARDS) – a review and proposed strategies toward a better understanding of pathogenesis, early diagnosis and therapy. Veterinary Ophthalmology 2016; 19: 319-331.
Return to SARDS RESOURCES Page





